When the FIFA World Cup kicks off in North America this month, the focus will be on the spectacle: the flags, the jerseys, the packed stadiums and sports bars and the once-in-a-generation chance for Canadian cities to host the world’s biggest sporting event.
But the less glamorous reality is that the World Cup is also a massive public health test. The 2026 tournament is the largest in FIFA history, bringing together 48 countries for 104 matches across 16 cities in Canada, the U.S. and Mexico. Canada is hosting 13 matches, six of them in Toronto, beginning June 12 with the first-ever men’s FIFA World Cup match on Canadian soil. Throughout the tournament, Toronto expects to attract about 300,000 out-of-town visitors, in addition to the 716,000 locals who plan to attend one or more live games. Vancouver, the other Canadian host city, is also expecting huge crowds; there, the projected number of visitors is closer to 350,000 people, plus the 385,000 locals who plan to attend at least one game.
That many people moving through that many cities is exactly the kind of thing that keeps infectious disease experts on alert. “You have this convergence of populations from around the globe that may be bringing microbes with them that happen to be in their particular area, and then at the actual site, there are opportunities for amplification,” says Dr. Kamran Khan, an infectious disease physician at St. Michael’s Hospital in Toronto and the founder and CEO of BlueDot, a Toronto-based artificial-intelligence software company.
Get our weekly newsletter – the people, places, and ideas revealing where Canada is headed.
Founded in 2013, BlueDot uses AI to monitor infectious disease threats around the world and help governments, health systems and companies assess what those threats could mean locally. Among the company’s self-stated wins: it signalled the global spread of Ebola in 2014 and a Zika virus outbreak in 2016, and it issued the first COVID-19 alert, beating the World Health Organization by several days.
In fact, BlueDot’s role in the pandemic became an early proof point for what AI-assisted outbreak surveillance can do. On Dec. 31, 2019, the company alerted its clients to a cluster of unusual pneumonia cases in Wuhan, China, days before major public-health agencies issued their own public warnings. It was able to predict the international spread of the virus to cities such as Bangkok, Tokyo, Seoul and Taipei before outbreaks occurred there.
Rather than “detecting” the virus in a lab, BlueDot’s platform scanned open-source signals, including international news reports and travel data, to identify a possible emerging threat and forecast where infected travellers were most likely to go next. Now, the company has clients across public health, defence, security, health care and the private sector, and it’s supporting various World Cup host cities, including Toronto, Vancouver and Kansas City.
Khan describes BlueDot’s work in three parts. The first is surveillance, or trying to make sense of scattered information from around the world. Some official systems track only certain notifiable diseases. Some issue delayed reports. Some places don’t have robust environmental surveillance, like wastewater monitoring. Then there are animal outbreaks, climate conditions, mosquito populations and online reports that may surface before official systems catch up.
“The first order of business is consolidating data that is highly unstructured, multilingual [and] coming in at different speeds and times,” says Khan, adding that BlueDot does this “every 15 minutes, 24 hours a day, 365 days a year.”
The second part of the company’s work is risk assessment. It isn’t enough to know that Ebola, measles or hantavirus is circulating somewhere. The practical question is: what is its significance here?
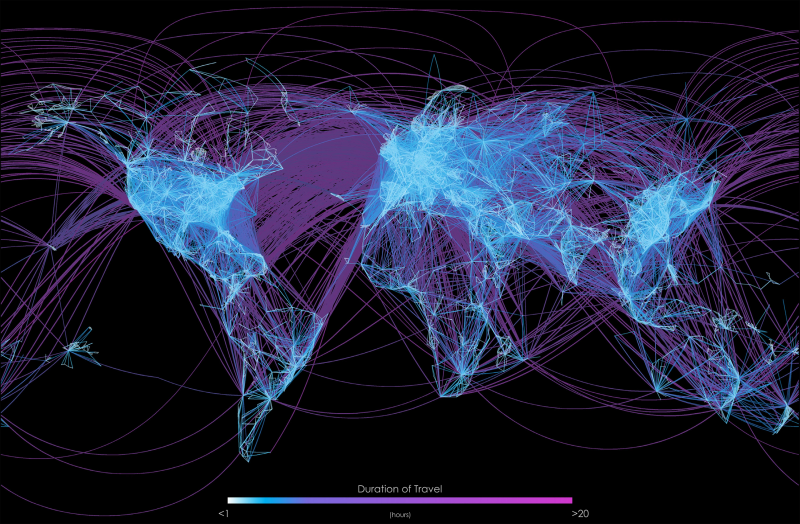
BlueDot uses a wide range of data – including, for example, tracking more than four billion commercial flight itineraries every year – to monitor how many people are travelling between borders and from where. The company uses this data to create a mobility map that correlates known outbreak locations with global flight paths, and it estimates the risk of disease importation to other cities or countries.
The third part is communication. After consolidating global surveillance data, BlueDot translates that information into formats for different audiences, including dashboards for public-health agencies and World Cup host cities, concise email briefings for executives or tailored alerts for health-care systems, pharmaceutical companies, security organizations and other private-sector clients. The point, Khan says, is to make complex data “consumable, understandable [and] actionable” for people who may not have a background in medicine, microbiology or epidemiology.
As an example, BlueDot assessed the 2022 FIFA World Cup in Qatar, where it focused on the top three disease threats as identified by in-house subject-matter experts. They included COVID-19, influenza and respiratory syncytial virus (RSV). Another instance is the company’s work around the Hajj, the annual pilgrimage for Muslims to Mecca that brings millions of people from around the world into dense settings over a short period of time. In its risk assessments, BlueDot identified a wide range of diseases that could be introduced, amplified or exported during the pilgrimage – including meningococcal disease, measles, dengue, malaria, cholera, Crimean-Congo hemorrhagic fever, yellow fever, Middle East respiratory symptom and seasonal influenza – all laid out into immediate risk, versus sporadic and long-term risk.
Here, Khan says, the promise of AI is scale. No human team could manually monitor every relevant signal, in every language, at every hour of the day. But Khan is also careful not to frame the technology as a magic machine that’s making decisions on its own; the company uses subject-matter experts and open-source intelligence practices to verify what its systems are seeing. “We aren’t just letting machines run away with this,” he says. “We go through verification: is this actually accurate? Is this not?”
Heading into the World Cup, BlueDot is most concerned about measles, an extremely contagious disease that has surged in recent years as vaccination rates have declined. In Canada and the U.S., public-health officials have reported ongoing measles activity in 2026, while the Pan American Health Organization has urged countries preparing for the World Cup to strengthen measles surveillance and vaccination efforts. Risks such as Ebola and hantavirus are also being monitored.
Still, there are limits to AI models, which can track people moving between countries and changing incidence rates but not necessarily interactions before symptoms appear. AI-powered disease surveillance is only as strong as the data feeding it. These systems can help public-health officials spot patterns faster, but they may also miss outbreaks in places with limited testing, poor reporting infrastructure, language barriers or restricted access to reliable public-health information. They can also overemphasize signals from regions with more media coverage or stronger digital footprints, while undercounting communities that are less visible online.
Carolyn McGregor, director and Canada Research Chair at the Joint Research Centre in AI for Health and Wellness at Ontario Tech University in Oshawa, Ont., cautions against over-reading the data: if cases rise during or after the World Cup, the tournament may be a factor, but it may not be the only one. There are also privacy concerns, says McGregor: while AI tools use public data to make general inferences and extrapolations, when the number of people in a particular population or location is low, identification can become easier.
For her, AI requires key safeguards that include transparency, oversight and humility, which means being clear about what the data shows, what it doesn’t and what assumptions are being built into any analysis.
For the average fan, the takeaway is to remember that public health at a mass event isn’t just a government problem and a tech problem but also one centred on human behaviour. McGregor says people can reduce their own risk by being mindful of their well-being, especially at an event where many will be travelling, drinking, staying out late and packing into crowded spaces. And according to Khan, this picture must involve health departments, governments, businesses and the public understanding that microbes move because people move.
“Ultimately, it’s global awareness and local readiness,” he says. “This is a whole-of-society challenge. We often just look to government, but the reality is every one of us has a part to play.”
At the World Cup, that may mean an AI-powered disease-surveillance company watching global signals in real time. But it also means public-health teams preparing hospitals, alerting frontline workers and encouraging vaccination, and fans staying home when they’re sick, washing their hands, checking their vaccinations and thinking twice before powering through symptoms in the name of the game.
Because the World Cup is, by design, a celebration of worldwide connection. In 2026, that connection is also the risk.