
Back in 2006, when Dr. Heather Ross was just 200 metres away from summiting the tallest mountain in Antarctica, she suddenly couldn’t breathe.
The Toronto-based clinical cardiologist was climbing Mount Vinson with Test Your Limits, the organization she’d founded to raise money for cardiovascular research, when she developed high-altitude pulmonary edema. The life-threatening condition is caused by excess fluid in the lungs, resulting in severe shortness of breath. It feels remarkably like heart failure, something that Ross has dedicated her career to treating at Toronto’s Peter Munk Cardiac Centre, part of the University Health Network (UHN). “I had what my patients get,” Ross says, “and until that moment I had no clue what it really felt like to not be able to breathe.”
After her near-death experience, Ross became singularly focused on understanding and improving heart failure patients’ quality of life. “I only had to feel it for hours,” she recalls. “I have patients that live with it for years.”
Get our weekly newsletter – the people, places, and ideas revealing where Canada is headed.
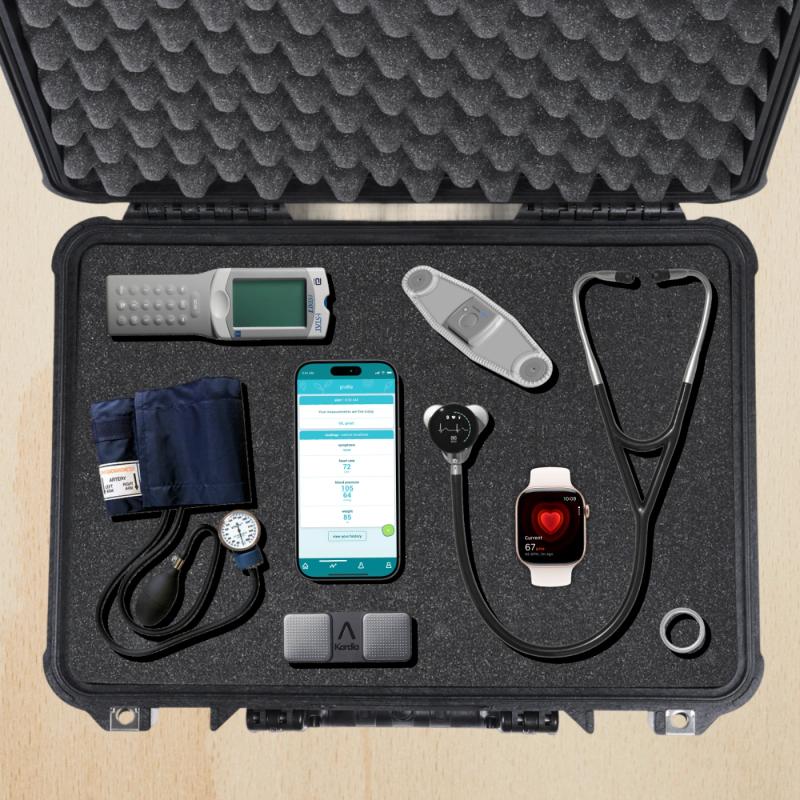
In the two decades since, Ross has brought the boundary-pushing drive that fuels her fundraising climbs (Test Your Limits has raised more than $4 million) to innovations for cardiac patients. Recently she developed what she calls a “hospital in a Pelican case,” referring to the hard-shell container used by photographers and others to transport fragile equipment. Ross fills these durable cases with digital tools that bring UHN’s world-class cardiology labs to patients who live far from their specialist’s office in downtown Toronto.
In heart failure, the organ is unable to pump enough blood to fuel the body. One in five Canadians will develop it in their lifetime, and cardiovascular disease is now the top non-communicable cause of death worldwide. It’s also a strain on our health-care system, costing more than $30 billion annually.
Heart failure rates are twice as high in northern Ontario than in the rest of the province. That is partly because about a third of the province’s Indigenous people live in its northern reaches, and Indigenous Canadians are at higher risk of cardiovascular disease – because of factors including oppression, racism, health-care biases and social disparity.
Another big factor is the long distances northerners have to travel to get specialized care.
Ross, who recently returned home after spending six days running a clinic in Sioux Lookout in northwestern Ontario, says cardiac patients in these communities have to take multiple flights between their homes and downtown Toronto. “If you’re a patient in Sandy Lake and you’re told to just pop on down to Toronto to get a test done ... that’s two full days of travelling in order to go there and back.”
Ross and her team routinely travel four to six times a year to spend a week or so seeing patients in northern communities. But it used to be that once they were onsite, they wouldn’t have access to the same high-end equipment available at UHN. So Ross began to build her “hospital in a Pelican case.”
It contains Health Canada-approved portable versions of the tools she and her colleagues use at the Peter Munk Cardiac Centre – including a blood analyzer called i-STAT, an Apple Watch and its suite of heart-monitoring apps, a digital stethoscope that allows doctors to hear heart sounds remotely, an electrocardiogram (ECG) machine the size of a USB key, and a portable ultrasound machine that is able to send images to a distant doctor to diagnose heart failure. Notably, all these tools have also been vetted to ensure they include privacy and safety guardrails.
“The goal is to be able to go to a community with my Pelican case and be who I am in Toronto,” Ross says. She adds that UHN hopes to start leaving the cases behind so that local nurses can use the tools after the Toronto doctors go back south. “It’ll help us triage better, make decisions about who needs to be transported out of the community and who can stay. Coupling this with virtual visits and in-person visits, we can provide wraparound care.”
About a decade ago, Ross and other UHN researchers also developed Medly, a smartphone app that allows patients to input their weight, blood pressure and heart rate daily. Based on this information, Medly’s algorithm flags patients who need care to a UHN-affiliated nurse or directs those in immediate danger to their nearest hospital. Traditionally, heart-failure patients are seen in what Ross calls “episodes of care,” sporadic follow-ups every six months to a year – or when something goes wrong. Using a piece of tech most Canadians have in their pocket, the cardiologist can now track patients’ health between appointments.
Ross has used Medly and her Pelican case in partnership with the Weeneebayko Area Health Authority (WAHA), which serves remote communities near James Bay. She and her team visit periodically to run clinics, treat patients in their homes and train WAHA nurses on various tools.
Sandra Kioke, WAHA’s senior vice-president and chief nurse executive, says that because of the visits and technology from Ross and her team, “patients don’t feel as alone. Instead of a cardiologist in Toronto they see twice a year or once a year, they have an ongoing trusted relationship.”
The Pelican case and Medly help keep people suffering from heart disease in their homes. “Without the tools that Heather and her team bring, patients may languish in their community and have to be medevaced out if their health has spiralled to a place where it can no longer be managed [locally],” adds Kioke. “For people that live in remote communities, not having to travel for care is very meaningful, and it could only be made possible through this group, who are 100-per-cent committed to addressing some of the health inequities that people have experienced up here for decades.”
Ross, a Member of the Order of Canada since 2020, acknowledges that while building more hospitals is an important part of increasing access to health care, it’s impossible to have one in every community. And that’s why digital tools to extend the reach of large hospitals are so important.
“We want to give the best care” she says. “We want to make sure that the access to [it] is equitable across all the different ways we think of equity, and we want to make sure that we are meeting patients where they’re at.”



